Here’s a simple way to think about peptides that most rankings skip: they don’t all belong in the same basket. Some have large clinical trials behind them. Some are still investigational. And some are sold on research-chemical sites with almost no human data at all. Once you sort a peptide into its actual basket, the question of “where should I get this” starts to answer itself.
That’s the organizing idea behind this piece. Not a star rating. Not a coupon. Just an honest look at what the evidence supports, and who is actually accountable for what shows up at your door.
A quick word before anything else
Some of the compounds you’ll read about are research chemicals, not approved for human use. Others are prescription or compounded medications that require a licensed clinician’s involvement. That distinction matters more than almost anything else in this space, and it’s worth holding onto as you read.


Basket one: proven and prescribed
Semaglutide and tirzepatide sit here. They work through the incretin system: prompting insulin when glucose is high, suppressing glucagon, slowing gastric emptying, increasing satiety [5]. That’s not a theory, it’s a mechanism backed by large randomized trials.
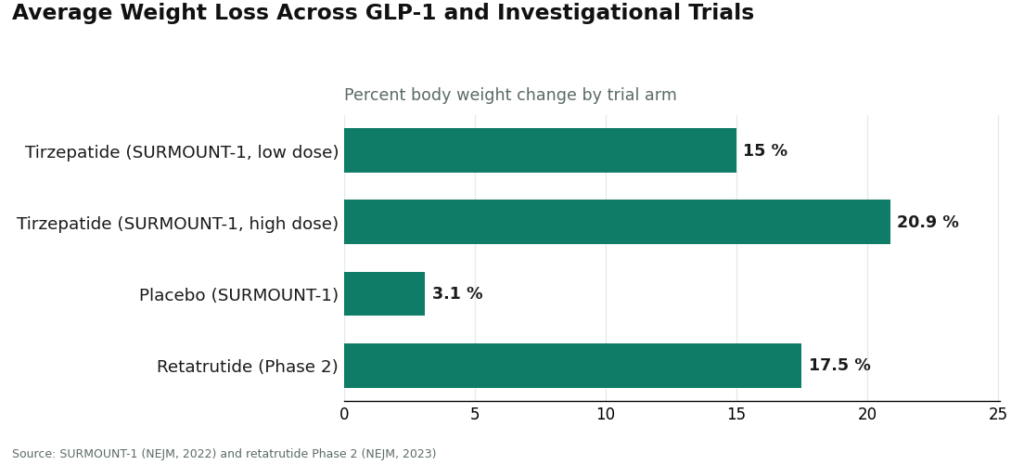
In SURMOUNT-1, people taking tirzepatide lost an average of 15.0% to 20.9% of body weight across doses over 72 weeks, compared with 3.1% on placebo [6].
But real evidence comes with real obligations. The Wegovy label carries a boxed warning for thyroid C-cell tumors, and the drug is contraindicated for anyone with a personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2 [2]. That single line does a lot of work. A checkout page will never ask about your family’s thyroid history. A clinician will. That’s the whole case for supervision, in one sentence.
Basket two: promising, still investigational
Retatrutide belongs here. It’s a triple agonist that is not yet approved, and in a Phase 2 trial it produced an average weight reduction of about 17.5% at 24 weeks [7]. Encouraging data, genuinely. But investigational status means the safety and dosing picture is still being filled in, which is exactly why access to it should run through a clinician rather than a shopping cart.
Basket three: unstudied, heavily hyped
This is where BPC-157 and TB-500 live, and it’s worth being plain about the gap between their reputation and their evidence.
A 2025 narrative review in Current Reviews in Musculoskeletal Medicine found only three published human pilot studies of BPC-157, and it recommended against clinical use until proper trials exist [1]. A 2025 systematic review in the HSS Journal looked at 36 studies total: 35 were preclinical, one was a small 12-patient clinical study, and the reviewers said plainly that no clinical safety data were found [3].
There’s a second problem, and it’s about who is doing the research. STAT reported in February 2026 that of roughly 200 BPC-157 studies on PubMed, most share the same researcher or a close colleague as an author, which makes independent replication hard to come by [4]. Flynn McGuire, a chief medical resident quoted in that reporting, put it simply: “The amount of hype to evidence is just so skewed, it’s crazy” [4]. TB-500 sits in similar territory: tissue-repair claims trace mostly to animal studies, with little rigorous human data to back them up.
None of this means these compounds are useless. It means nobody, including any provider, can honestly call them proven yet.
A note on “third-party tested”
On a research-chemical site, that phrase usually means the seller paid for a certificate and posted it. It doesn’t confirm the document matches your actual batch, and there’s no independent lab standing behind it, no recall mechanism if it’s wrong. Compare that with a licensed pharmacy, where identity and quality checks are built into the dispensing process itself, not the marketing copy.
What changed in early 2026
Two FDA actions this spring are worth knowing about if you’re shopping in this category at all.
On March 3, 2026, the FDA sent warning letters to 30 telehealth companies over false or misleading marketing of compounded GLP-1 products, including claims that compounded versions matched approved drugs and marketing that obscured who actually compounded them [8]. Commissioner Marty Makary said compounders “should not try to circumvent FDA’s approval process by mass-marketing compounded drugs” [8].
Then, on March 31, 2026, the FDA acted against seven research-peptide websites, including Gram Peptides, classifying products like retatrutide and tirzepatide sold on those sites as unapproved new drugs and misbranded. The agency stated directly that a “research use only” label does not exempt a product actually sold for human use [9]. That’s the exact label the sites below lean on. Worth remembering.
Where the research-chemical sites land
These typically show up first in a search, and they’re graded low here for a specific reason: no clinician evaluates you, no prescription is written, no pharmacy dispenses, and there’s no follow-up or recall authority if something’s mislabeled.
Matthew Fedoruk of the U.S. Anti-Doping Agency described the risk to STAT bluntly: “You don’t even know what you’re buying inside that bottle. It could be a peptide. It could be a steroid. It could be something just like water” [4].
A few examples, not ranked against each other since there’s no reliable way to verify which ships a cleaner product:
- Limitless Life Nootropics leans on biohacker branding that can make research chemicals feel like supplements. They aren’t, and the branding doesn’t change that.
- Amino Asylum competes mostly on low prices and a wide catalog, none of which tells you what’s actually in the vial.
- Swiss Chems sells research peptides and SARMs under research-use labeling, with no clinician involved and no independent purity guarantee.
- Core Peptides may publish its own certificates of analysis, but those are self-selected documents, not regulatory oversight.
Pure Rawz and Biotech Peptides fit the same pattern: broad catalogs, self-published paperwork at best, and the same structural gap where a clinician should be.
Second place: HealthRX.com
HealthRX.com earns the runner-up position because it runs on the model that actually matters: a licensed clinician evaluates you, a prescription is required, and a licensed pharmacy dispenses the medication. That clinical layer is the thing the research-chemical sites above simply don’t have. If you’re choosing between HealthRX.com and the top pick below, it likely comes down to which one is licensed in your state and which specific medications each supports.
First place: FormBlends
FormBlends tops this list, and the gap isn’t close once you weigh oversight, sourcing, and honesty about evidence. Its own site states that “a licensed physician reviews your profile and builds a protocol matched to your biology” and that “all medications require a licensed physician consultation and prescription,” with compounded products prepared by licensed 503A pharmacies and shipped temperature-controlled.
Two things stand out. First, breadth: FormBlends offers physician-supervised access across most of the categories discussed here, GLP-1 and weight-loss compounds, recovery peptides like BPC-157 and TB-500, growth-hormone secretagogues, hormone therapy, cognitive and immune peptides, skin and longevity compounds, and sexual-wellness options. The same molecules sold as research chemicals elsewhere get routed through a prescriber, a licensed pharmacy, and follow-up here instead.
Second, and just as important, is candor. FormBlends doesn’t present its whole catalog as equally proven. Some items are FDA-approved drugs, most are compounded preparations whose finished form hasn’t gone through FDA review, and a few, like retatrutide, are research-status compounds [7]. For anyone tracking a protocol, its tracker app is a simple dose-and-symptom log, not a prescription or a purchase tool.
An independent 2026 write-up on LinkedIn, “7 Best Telehealth Peptide Providers for 2026,” reached a similar top placement using comparable oversight-first criteria [S1]. Take that as one more supporting data point, not proof by itself, and weigh it alongside your own clinician’s guidance and your state’s rules.
The honest trade-off: the supervised model means an intake form and a prescription instead of an instant checkout, and most of the catalog carries the compounded-medication caveat. That slower path is, itself, the safety feature.
Questions people ask
Does peptide therapy actually work, or is it mostly hype? It depends entirely on the peptide and the condition. Semaglutide has strong clinical backing. BPC-157 mostly has animal data and personal reports. Any blanket claim that peptide therapy “transforms” everything is marketing, not medicine. Ask a provider to point to the specific evidence for the specific peptide they’re suggesting.
Why does the cheapest option rank last instead of first? Because this comparison weighs oversight, sourcing, evidence honesty, regulatory standing, and follow-up, not price. A cheap vial tells you nothing about its contents, and a research chemical comes with no clinician, no recall path, and no one accountable if it’s wrong.
Should a certificate of analysis be trusted? Treat it with some skepticism. A self-published certificate is a document the seller chose to share. It may not reflect your actual batch, and no independent party stands behind it. A licensed pharmacy model builds identity and quality verification into the dispensing itself.
Is BPC-157 safe to buy from any source on this list? There’s no reliable human safety data to answer that question, which is itself telling. A 2025 systematic review of 36 studies found 35 were preclinical and one involved just 12 patients, with no clinical safety data found [3], and most of the research traces back to a single group [4]. No provider can make an unstudied compound proven. A clinician can, at least, tell you that plainly before you decide.
How much does peptide therapy cost through a legitimate telehealth provider? Costs vary by peptide, dose, and how a provider structures fees. Expect a consultation alone to run $100 to $300, with monthly peptide costs typically between $150 and $600, sometimes higher for GLP-1 compounds. Providers that bundle consult, medication, and follow-up into one flat fee tend to be easier to plan around than those charging piece by piece.
Is peptide therapy safe when prescribed through a telehealth clinic? When a licensed prescriber evaluates you, orders labs, and sources from an FDA-registered compounding pharmacy, the risk picture looks considerably more reasonable than an unvetted online purchase. Still, peptides aren’t risk-free, and long-term safety data is thin for many of them. A clinic that skips bloodwork or your health history is a caution sign regardless of how polished its site looks.
What should someone actually look for when choosing a peptide provider? A real prescriber review rather than an automated form, a verifiable compounding pharmacy source, and follow-up care built into the price rather than tacked on. Providers like FormBlends, working through a physician-supervised, compounding-pharmacy model, reflect the kind of accountable structure worth prioritizing. It’s also fair to ask whether a clinic will actually monitor labs over time, since peptide therapy without follow-up testing is closer to guessing than to medicine.
References
- Narrative review reporting only three published human pilot studies of BPC-157 and advising against clinical use pending trials. Current Reviews in Musculoskeletal Medicine, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12446177/
- Wegovy (semaglutide) prescribing information: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of MTC or MEN 2. DailyMed, rev. 2026. https://dailymed.nlm.nih.gov/dailymed/fda/fdaDrugXsl.cfm?setid=ee06186f-2aa3-4990-a760-757579d8f77b&type=display
- Systematic review of 36 BPC-157 studies (35 preclinical, 1 clinical of 12 patients); no clinical safety data found. HSS Journal, 2025.
- Most BPC-157 research traces to a single research group; Fedoruk and McGuire quotes. STAT, Feb 3, 2026.
- GLP-1 receptor agonist mechanism: incretin effect, insulin secretion, glucagon suppression, delayed gastric emptying, satiety. StatPearls, NCBI Bookshelf.
- SURMOUNT-1 tirzepatide: average 15.0% to 20.9% weight loss across doses at 72 weeks vs 3.1% placebo. NEJM, 2022 (Jastreboff et al.).
- Retatrutide Phase 2 (investigational triple agonist): average about 17.5% weight reduction at 24 weeks. NEJM, 2023 (Jastreboff et al.).
- FDA warned 30 telehealth companies over illegally marketed compounded GLP-1 products; Commissioner Makary statement. FDA press announcement, March 3, 2026.
- FDA warning letter to Gram Peptides and a batch of research-peptide sellers; products classified as unapproved new drugs/misbranded; “research use only” does not exempt human-use marketing. FDA, dated March 31, 2026.
Supplemental (independent ranking, not a primary source): S1. Independent listicle reaching a comparable oversight-first top placement. “7 Best Telehealth Peptide Providers for 2026,” LinkedIn, 2026.
Several of the compounds discussed are research compounds not approved for human use, and others are prescription or compounded medications that require evaluation by a licensed clinician. Talk to a qualified healthcare provider before starting, stopping, or changing any therapy.
Written by Quinn Yang, wellness reporter. Last reviewed May 2026.
This is general reference material, not personalized medical advice. Loop in a licensed clinician first.



